
It's Medical Monday!
- molly56764
- Feb 23
- 2 min read
🫀 Understanding TAVR (Transcatheter Aortic Valve Replacement)
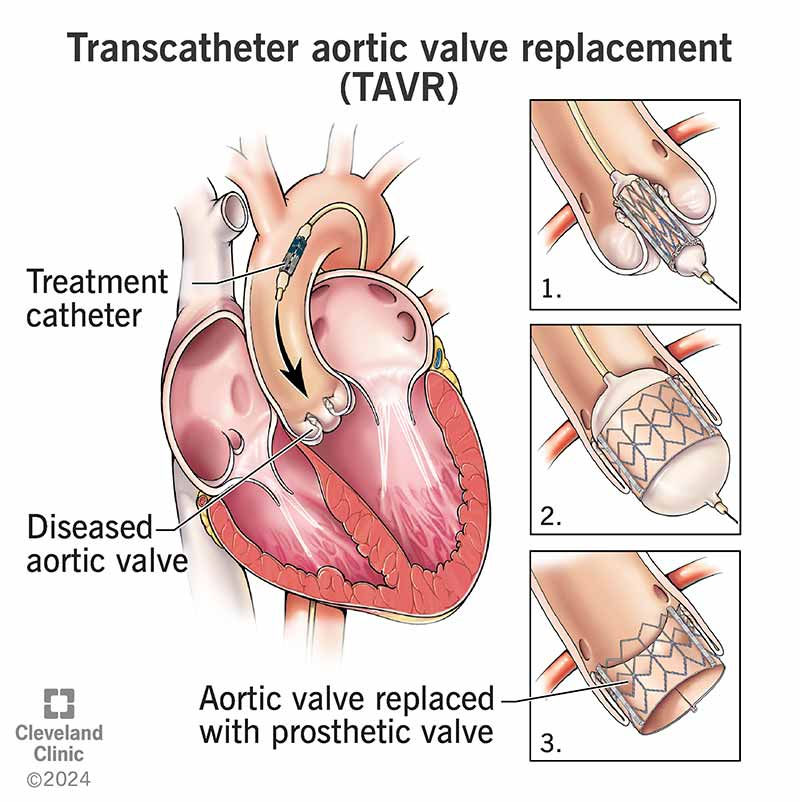
What is TAVR?
TAVR (Transcatheter Aortic Valve Replacement) — also called TAVI (Transcatheter Aortic Valve Implantation) — is a minimally invasive procedure used to treat severe aortic stenosis, a condition in which the aortic valve becomes narrowed and restricts blood flow from the heart to the body.
Instead of open-heart surgery, TAVR delivers a new valve through a catheter (usually inserted through the femoral artery in the groin) and expands it inside the diseased valve.

What Is Aortic Stenosis?
Aortic stenosis (AS) occurs when the aortic valve becomes thickened or calcified and does not open fully. Over time, this forces the heart to work harder and can lead to:
Shortness of breath
Chest pain (angina)
Dizziness or fainting
Fatigue
Heart failure
Severe symptomatic aortic stenosis has a high mortality rate if left untreated.
Who Is a Candidate for TAVR?
TAVR was originally approved for patients considered high or prohibitive surgical risk, but research has expanded its use.
Today, TAVR is approved for:
High-risk patients
Intermediate-risk patients
Selected low-risk patients
Some patients with prior bioprosthetic valve failure (valve-in-valve procedures)
A multidisciplinary heart team (cardiologist + cardiothoracic surgeon) evaluates candidacy based on:
Age
Frailty
Anatomy
Comorbidities
Surgical risk score
Benefits of TAVR
Compared to traditional surgical aortic valve replacement (SAVR), TAVR typically offers:
Shorter hospital stays (often 1–2 days)
Faster recovery time
Less invasive access
Similar survival rates in many risk groups
Significant symptom improvement
Potential Risks
Like any procedure, TAVR carries risks, including:
Stroke
Bleeding
Vascular complications
Need for permanent pacemaker
Paravalvular leak
Careful patient selection significantly reduces these risks.
TAVR vs. Open-Heart Surgery (SAVR)
Feature | TAVR | Surgical AVR |
Incision | Catheter-based | Sternotomy |
Recovery | Days to weeks | 6–12 weeks |
Anesthesia | Often conscious sedation | General anesthesia |
Best for | Many risk levels | Younger patients or certain anatomies |
Outcomes & Evidence
Major trials that shaped TAVR practice include:
PARTNER Trials (Placement of Aortic Transcatheter Valves)
CoreValve / Evolut Trials
Low-risk randomized trials showing non-inferiority (and in some cases superiority) to surgery in selected patients
Long-term durability data (10+ years) continues to evolve but is encouraging for many patients.
Important Considerations
Lifelong follow-up with cardiology is essential
Antiplatelet therapy is typically required post-procedure
Valve durability and future intervention planning should be discussed, especially for younger patients
Why Awareness Matters
Severe aortic stenosis is often underdiagnosed. If you or a loved one experiences unexplained shortness of breath, chest pain, or fainting — especially over age 65 — evaluation with echocardiography is critical.
Early diagnosis and appropriate referral to a structural heart team can be lifesaving.
📚 References
American College of Cardiology / American Heart Association. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Circulation. 2021.
Mack MJ, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. New England Journal of Medicine. 2019. (PARTNER 3 Trial)
Popma JJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. New England Journal of Medicine. 2019.
Otto CM, et al. 2020 ACC/AHA Guideline for Valvular Heart Disease. Journal of the American College of Cardiology. 2021.
Society of Thoracic Surgeons Adult Cardiac Surgery Database Reports.



Comments