
It's Topic Tuesday!
- Alvaro Jose Martinez Santacruz
- May 12
- 4 min read
Updated: May 24
Hello, everyone! I hope you are all doing well. My name is Alvaro, and today our discussion focuses on acute Type B aortic dissection (TBAD), which occurs when a tear develops in the descending thoracic aorta, allowing blood to enter the aortic wall and create a false lumen.
This false channel can compress the true lumen, reducing blood flow to critical branch vessels—and when organs lose perfusion, malperfusion syndrome develops.
This is one of the most dangerous complications of aortic dissection.
What is a Type B aortic dissection?
A Type B aortic dissection occurs when a tear develops in the inner layer of the descending thoracic aorta, allowing blood to enter the wall of the vessel and split its layers apart. This creates two channels for blood flow: the true lumen, which is the normal pathway, and the false lumen, an abnormal channel formed within the aortic wall. As blood continues to flow into this false lumen, it can expand and compress the true lumen, reducing blood flow to important branch vessels. When these branches supply organs such as the intestines, kidneys, or lower limbs, this reduced perfusion can lead to malperfusion syndrome, causing tissue ischemia and potentially life-threatening organ dysfunction.
🧠 A Simple Analogy
Think of the aorta like a one-lane highway. Suddenly, a wall breaks and traffic spills into a new unauthorized lane. This new lane (false lumen) becomes crowded and pushes into the original lane (true lumen), narrowing it. Cars trying to exit toward important destinations—like the kidneys, intestines, or legs—can no longer get through.
That traffic jam is malperfusion.

📍 What Makes It “Type B”?
Aortic dissections are classified using the Stanford system:
Type A → involves the ascending aorta (surgical emergency).
Type B → begins distal to the left subclavian artery, involving the descending thoracic aorta.
Non-A Non-B dissection → involves the aortic arch without classic ascending aortic involvement, representing a more complex and evolving category.
Among these, Type B dissections are particularly important because they may initially appear stable, but can rapidly become life-threatening when branch vessel perfusion is affected.
⚠️ Malperfusion Syndrome: When Branches Lose Blood Flow
A major complication of Type B dissection is malperfusion syndrome, which occurs when the dissection flap obstructs branch vessels and reduces blood flow to vital organs. Depending on the arteries involved, patients may develop visceral malperfusion, leading to severe abdominal pain and gut ischemia; renal malperfusion, causing oliguria and acute kidney injury (AKI); or lower limb malperfusion, presenting with pain, coldness, pulselessness, and signs of acute limb ischemia. This transforms an uncomplicated dissection into a complicated emergency, requiring rapid recognition and treatment to prevent irreversible organ damage.
🔎 Diagnostics: How Do We Identify and Assess It?
Diagnosis begins with clinical suspicion, especially in patients presenting with sudden chest, back, or abdominal pain, pulse deficits, or signs of end-organ ischemia. The gold-standard diagnostic test is Computed Tomography Angiography (CTA), which provides rapid visualization of the intimal tear, differentiates the true and false lumen, and evaluates branch vessel involvement, the extent of dissection, and signs of rupture or malperfusion.
Additional diagnostic tools may include:
Laboratory markers, such as elevated lactate (suggesting visceral ischemia), rising creatinine (renal malperfusion), and metabolic acidosis
Physical examination, assessing pulse asymmetry, neurologic deficits, or limb ischemia
Transesophageal echocardiography (TEE) is useful in unstable patients or when CTA is not immediately available.
Combining imaging findings with clinical symptoms is crucial, since the anatomy of the dissection alone does not always predict the severity of organ compromise.
🛠️ How Is Type B Aortic Dissection Managed?
Management depends on whether the dissection is uncomplicated or complicated by malperfusion, rupture, or persistent pain. The goal is to reduce aortic stress, prevent progression, and restore blood flow when branch vessels are compromised.
Conservative Medical Management
Reserved for uncomplicated Type B dissections, initial treatment focuses on anti-impulse therapy:
Strict blood pressure control (target SBP 100–120 mmHg)
Heart rate reduction (goal <60 bpm, usually with IV beta-blockers)
Adequate pain control
Close ICU monitoring and serial imaging surveillance
This strategy aims to reduce shear stress on the aortic wall and prevent extension of the dissection.
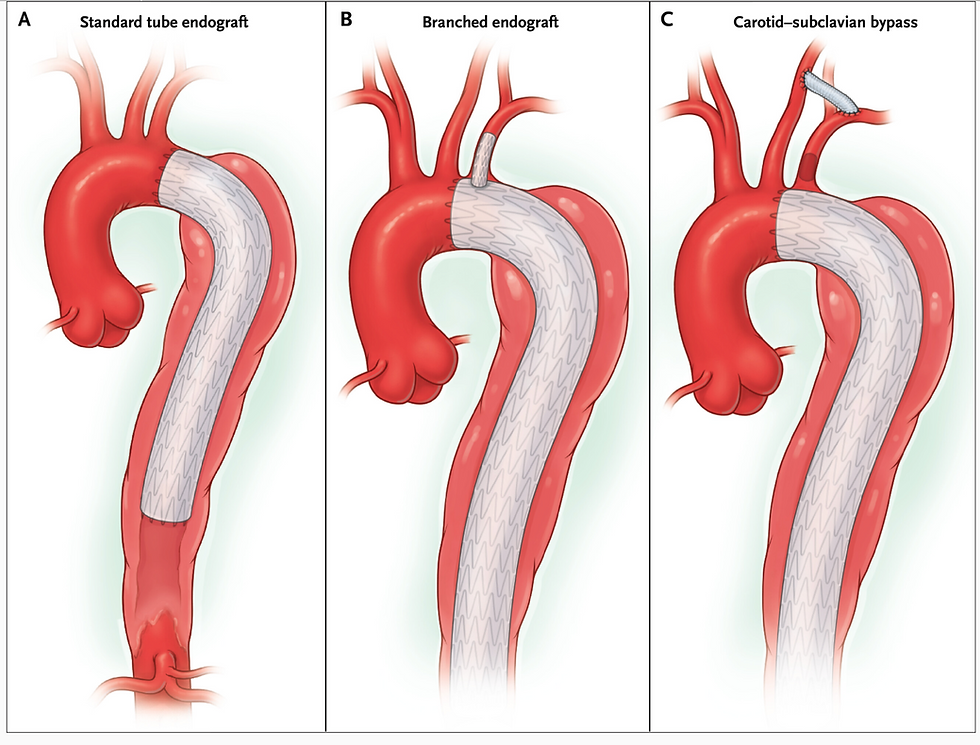
Endovascular Management (TEVAR)
For many complicated Type B dissections, thoracic endovascular aortic repair (TEVAR) is the preferred intervention.
TEVAR works by:
Covering the primary intimal tear
Redirecting blood into the true lumen
Promoting false lumen thrombosis
Relieving dynamic branch vessel obstruction and restoring organ perfusion
It is often the first-line treatment when malperfusion syndrome develops.
Additional Branch Vessel Intervention
In some patients, restoring aortic flow alone is not enough—especially when there is static obstruction of branch vessels.
Additional procedures may include:
Branch vessel stenting
Fenestration techniques
Surgical bypass in selected complex cases
These are used to directly re-establish perfusion to affected organs or limbs.
Long-Term Management Also Depends On
⚡ Presence of complications: Malperfusion, rupture risk, refractory pain, or rapid aortic expansion often determines the urgency of intervention.
📊 Imaging surveillance: Lifelong follow-up with CTA or MRA is essential to monitor aortic remodeling and detect aneurysmal degeneration.
🧬 Underlying aortic pathology: Connective tissue disorders, or atypical patterns, such as non-A/non-B dissections, may influence procedural choice and long-term strategy.
The ultimate goal is not only to survive the acute dissection but to prevent future complications through careful surveillance and tailored intervention.
🧠 Key Takeaway
💡 Type B aortic dissection is not just a structural disease—it is a flow disease. The main danger is not the tear itself, but how it disrupts circulation and leads to malperfusion syndrome, transforming a stable condition into a multi-organ emergency.
👉 Recognize early
👉 Image promptly
👉 Restore flow before ischemia becomes irreversible
💡 Fun Fact
The concept of “false lumen thrombosis” after TEVAR is considered a positive remodeling marker, meaning the aorta is biologically healing and stabilizing over time.
This is all we have for you today folks. We hope this has been informative. Join us back here next Tuesday
ATT
ALVARO JOSE MARTINEZ SANTACRUZ
Bibliography
Dieter, R. S., Dieter, R. A., Jr, & Raymond A. Dieter, I. I. I. (Eds.). (2019). Diseases of the aorta. Springer International Publishing.
Fiona, R., & K&, T. (2016, November 17). Type B dissections: What we know and what we don’t. Endovascular Today; Bryn Mawr Communications. https://evtoday.com/articles/2016-nov/type-b-dissections-what-we-know-and-what-we-dont
Harris, C. G., Croce, B., & Tian, D. H. (2014). Type B aortic dissection. Annals of Cardiothoracic Surgery, 3(3), 339. https://doi.org/10.3978/j.issn.2225-319X.2014.05.10
Mussa, F. F., & Kougias, P. (2025). Management of acute type B aortic dissection. The New England Journal of Medicine, 393(9), 895–905. https://doi.org/10.1056/NEJMra2405257



Comments