
It’s Medical Monday-Who's at Higher Risk for Aortic Disease?
- molly56764
- Jan 12
- 5 min read

Medical Monday: Who's at Higher Risk for Aortic Disease?
Welcome back to Medical Monday!
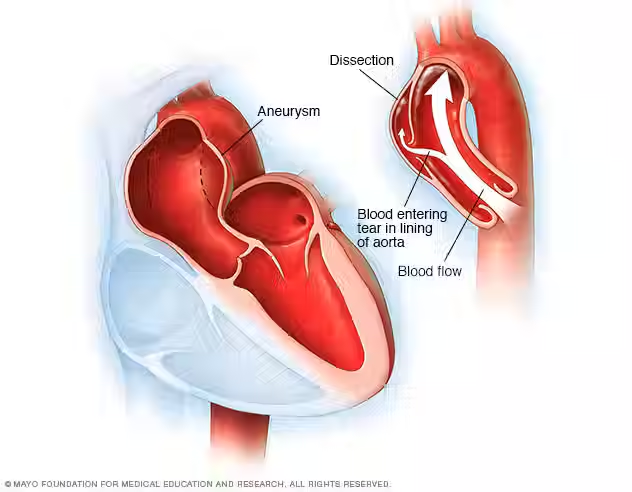
Today, we're discussing something that may be pertinent to many of us: who is at increased risk for aortic disease? Anyone can develop problems in their aorta, but certain conditions greatly elevate the risk of issues we often discuss, such as aortic aneurysms, dissections, and problems with the aortic valve, and accelerate the age at which these may present, compared to someone without such conditions.
Understanding these conditions and their associated risk factors will not only help you learn about your own anatomy but may also provide insight into what many of our other members at Aortic Hope live with daily. If you have one of these conditions yourself or if you have a family member affected by one of these conditions, this post will provide information on how important it is to undergo regular screening and what actions you can take to protect your aorta.
Connective Tissue Disorders
Marfan Syndrome
Marfan Syndrome is a genetic condition that affects a gene (FBN1) that is in part responsible for the body’s connective tissue. The connective tissue in the body acts like "glue," holding our tissues and organs together. Marfan syndrome is relatively rare in that it affects approximately 1 in 5000 people. Many will be tall, have long limbs, have flexible joints, and possibly other distinctive eye and skeletal features. A fun fact is that many people believe Abe Lincoln may have had Marfan.
Why does it cause problems with the aorta?
Like bones and skin, our vasculature also utilizes connective tissue, especially the aorta. Marfan patients have weakened connective tissue, which increases the likelihood of aortic wall stretching and potentially tearing. It is especially dangerous because the aortic root (the point where the aorta leaves the heart) is particularly susceptible, to the point that some young patients undergo aortic root surgery before these problems develop.
Loeys-Dietz Syndrome
Loeys-Dietz syndrome is a different genetic condition that affects the body’s connective tissue. It affects a group of 5 different genes instead of just 1, and is even rarer at approximately 1 in 50,000. While Loeys-Dietz syndrome is often confused with Marfan syndrome, it has several distinguishing characteristics. Individuals who suffer from Loeys-Dietz syndrome often exhibit wide-set eyes, a cleft palate, and a propensity to develop twisted arteries.
Why does it cause problems with the aorta?
Loeys-Dietz syndrome can result in more severe problems than Marfan syndrome. People with Loeys-Dietz syndrome are at higher risk for aortic dissection, a tear in the inner layer of the aorta, even when the aorta is smaller than in people with Marfan syndrome.
Ehlers-Danlos Syndrome (Vascular Type)
There are several forms of Ehlers-Danlos syndrome, but the vascular type (vEDS) is most relevant to the aorta. It has been hard to nail down exactly how prevalent vEDS is, but most studies put it somewhere between 1 in 20,000 and 1 in 50,000 people. Here, there is an issue with a gene involved in collagen production, which gives our body’s tissues strength. The primary symptoms of the vascular type of Ehlers-Danlos syndrome include fragile skin that may appear translucent, bruising easily, and fragile blood vessels. Because the blood vessels are so fragile, individuals with vEDS are at increased risk of experiencing an arterial dissection or rupture.
Connective Tissue Disease: What to Do:
● Get annual echocardiograms or cardiac MRIs to measure your aortic diameter.
● Managing blood pressure is critical to maintaining overall health because high blood pressure can be particularly dangerous.
● Do not engage in high-impact activities such as contact sports or heavy weight lifting.
Bicuspid Aortic Valve (BAV)
A BAV is a much more common condition where approximately 1–2% of the population is born with an aortic valve that has 2 leaflets instead of the typical 3. In fact, many individuals who are born with this condition will never learn of its existence!
How does it affect the aorta?
Individuals who are born with a BAV are at an 8 to 10-fold greater risk of developing an ascending aortic aneurysm than the general population. This increased risk results from how blood flows through the valve and from genetic factors that weaken the aorta's walls.
BAV: What to do:
● Perform echocardiography immediately after the diagnosis to assess the aorta’s size.
● Follow up with imaging studies at intervals your surgeon recommends; typically 1-2 years.
● Maintain blood pressure under strict control.
● Surgical repair of the aorta is usually indicated when the diameter exceeds a certain size (typically 5.5cm)
● Screen all first-degree relatives (parents, siblings, children) of an individual diagnosed with BAV.
3. Turner Syndrome.
Approximately 1 in 2500 females are born with Turner syndrome. Females and women with Turner syndrome are generally smaller in stature and may also have various congenital heart defects.
How does it affect the aorta?
Up to 40% of women with Turner syndrome have cardiovascular malformations, including a variety of anomalies such as a bicuspid aortic valve, coarctation of the aorta (narrowing), and an increased risk of aortic dissection, which is most commonly seen at the aortic root and ascending aorta. Here, the increased aortic risk stems from multiple factors, including hypertension, malformations, and aortic wall weakness, as we have seen previously.
Turner Syndrome: What to do:
● Conduct a comprehensive cardiac assessment in early childhood.
● Use regular imaging to monitor the aorta throughout the lifetime (minimum of every 2–3 years, but more frequently if there are abnormalities)
● Strict management of blood pressure is necessary because hypertension is a major risk factor for aortic disease.
● Women with Turner syndrome should receive special care during pregnancy, as their risk of experiencing aortic dissection increases significantly.
The Bottom Line: Screening Saves Lives
If you have any of these conditions, regular screening isn't optional; it's essential. The goal is to catch problems early, when they can be managed with medication or scheduled for surgery at the right time, rather than facing an emergency dissection or rupture.
💥Jack's Summary: Action Steps
If you have a high-risk condition:
1. Know your aortic measurements and keep track of changes over time.
2. Get appropriate imaging based on your condition (don't skip appointments!)
3. Control your blood pressure (this is one of the most important things you can do!)
4. Know your family history and encourage close relatives to get screened.
5. Work with specialists who understand your specific condition.
6. Avoid high-risk activities like heavy weightlifting, contact sports, or extreme straining.
7. Carry medical information about your condition, especially when traveling.
Have a great week,
Jack
References
● Milewicz DM, Braverman AC, De Backer J, Morris SA, Boileau C, Maumenee IH, Jondeau G, Evangelista A, Pyeritz RE. Marfan syndrome. Nature reviews Disease primers. 2021 Sep 2;7(1):64.
● Isselbacher EM, Preventza O, Black JH 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. J Am Coll Cardiol. 2022;80(24):e223-e393
● Gouda P, Kay R, Habib M, Aziz A, Aziza E, Welsh R. Clinical features and complications of Loeys-Dietz syndrome: a systematic review. International Journal of Cardiology. 2022 Sep 1;362:158-67.
● Frank M, Adham S, Seigle S, Legrand A, Mirault T, Henneton P, Albuisson J, Denarié N, Mazzella JM, Mousseaux E, Messas E. Vascular Ehlers-Danlos syndrome: long-term observational study. Journal of the American College of Cardiology. 2019 Apr 23;73(15):1948-57.
● Verma S, Siu SC. Aortic dilatation in patients with bicuspid aortic valve. New England Journal of Medicine. 2014 May 15;370(20):1920-9.
● Kostopoulou E, Bosdou JK, Anagnostis P, Stevenson JC, Goulis DG. Cardiovascular Complications in Patients with Turner’s Syndrome. Current Pharmaceutical Design. 2020 Dec 1;26(43):5650-9.


Comments